Clinical Studies Experience: Clopidogrel has been evaluated for safety in more than 44,000 patients, including over 12,000 patients treated for 1 year or more Clopidogrel 75 mg/day was well tolerated compared to acetylsalicylic acid (ASA) 325 mg/day in CAPRIE. The overall tolerability of clopidogrel in this study was similar to ASA regardless of age, gender and ethnicity. The clinically relevant adverse effects observed in CAPRIE, CURE, CLARITY, COMMIT and ACTIVE-A are discussed as follows.
Haemorrhagic disorders: In CAPRIE, the overall incidence of bleeding on clopidogrel and ASA was the same (9.3%). The incidence of severe cases was 1.4% and 1.6% in the clopidogrel and ASA groups, respectively.
In patients receiving clopidogrel, gastrointestinal bleeding occurred at a rate of 2.0% and required hospitalisation in 0.7%. In patients receiving ASA, the corresponding rates were 2.7% and 1.1%, respectively.
The overall incidence of other bleeding disorders was higher in the clopidogrel group (7.3%) compared to ASA (6.5%). However, the incidence of severe events was similar in both treatment groups (0.6% vs. 0.4%). The most frequent events reported were purpura/bruising and epistaxis. Other less frequently reported events were haematoma, haematuria and eye bleeding (mainly conjunctival).
The incidence of intracranial bleeding was 0.4% for clopidogrel compared to 0.5% for ASA.
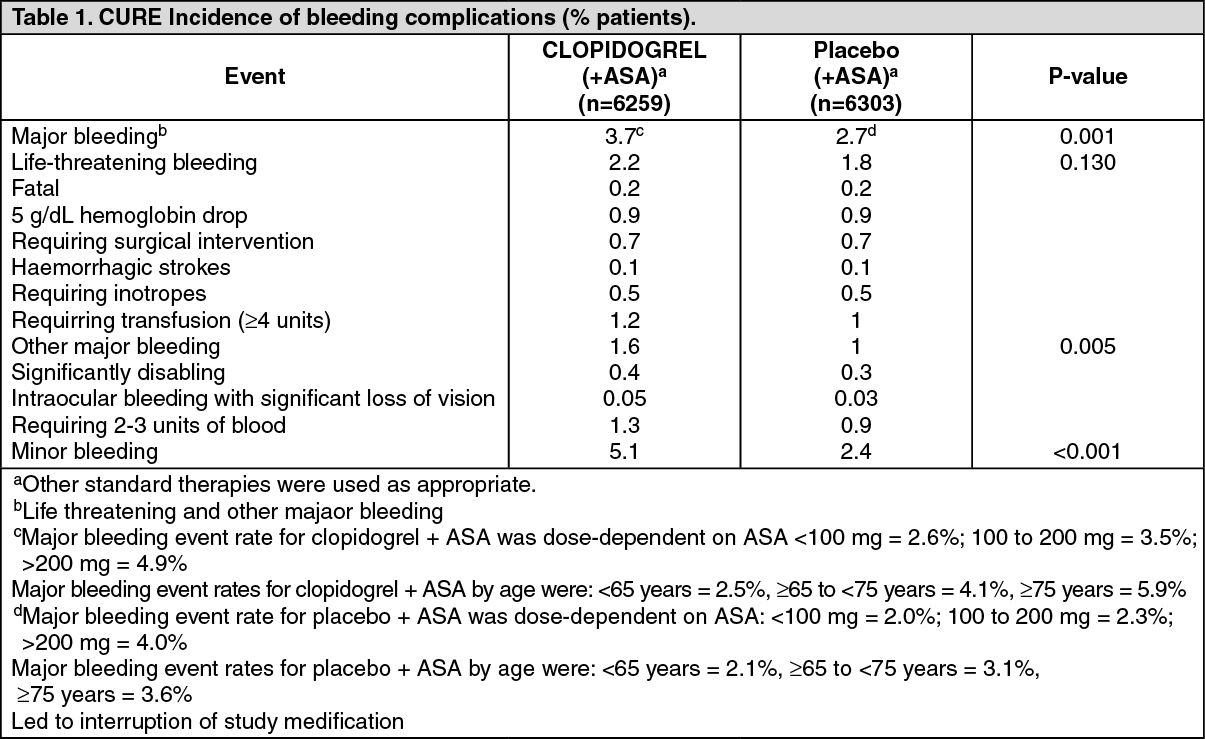
In CURE, there was an increase in major and minor bleeding between the clopidogrel + ASA group compared with the placebo + ASA group (event rates 3.7% vs. 2.7%, for major, respectively, and 5.1% vs. 2.4% for minor). The principal sites for major bleeding included gastrointestinal and at arterial puncture sites.
The increase in life-threatening bleeding in the clopidogrel + ASA group compared to the placebo + ASA group was not statistically significant (2.2% vs. 1.8%). There was no difference between the two groups in the rate of fatal bleeding (0.2% in both groups). The rate of non-life-threatening major bleeding was significantly higher in the clopidogrel + ASA group compared with the placebo + ASA group (1.6% vs. 1%), and the incidence of intracranial bleeding was 0.1% in both groups.
The major bleeding event rate for clopidogrel + ASA was dose-dependent on MA (<100 mg: 2.6%, 100-200 mg. 3.5%; >200 mg: 4.9%) as was the major bleeding event rate for placebo + ASA (<100 mg: 2.0%; 100-200 mg: 2.3%; >200 mg: 4.0%).
There was no excess in major bleeds within 7 days after coronary bypass graft surgery in patients who stopped therapy more than five days prior to surgery (4.4% clopidogrel + ASA vs. 5.3% placebo + ASA) In patients who remained on therapy within five days of bypass graft surgery, the event rate was 9.6% for clopidogrel + ASA, and 6.3% for placebo + ASA. The overall incidence of bleeding is described in Table 1 for patients receiving both clopidogrel and ASA in CURE.
Ninety-two percent (92%) of the patients in the CURE study received heparin/LMWH. and the rate of bleeding in these patients was similar to the overall results. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In CLARITY, the incidence of major bleeding (defined as intracranial bleeding or bleeding associated with a fall in hemoglobin >5 g/dL) was similar between groups (1.3% versus 1.1% in the clopidogrel + ASA and in the placebo + ASA groups, respectively). This was consistent across subgroups of patients defined by baseline characteristics, and type of fibrinolytics or heparin therapy. The incidence of fatal bleeding (0.8% versus 0.6% in the clopidogrel + ASA and in the placebo + ASA groups, respectively) and intracranial haemorrhage (0.5% versus 0.7%. respectively) was low and similar in both groups.
The overall rate of noncerebral major bleeding or cerebral bleeding in COMMIT was low and similar in both groups as shown in Table 2 as follows. (See Table 2.)
Click on icon to see table/diagram/image
In ACTIVE-A, the rate of major bleeding was greater in the clopidogrel + ASA group than in the placebo + ASA group (6.7% versus 4.3%). Major bleeding was mostly of extracranial origin in both groups (5.3% in the clopidogrel+ASA group; 3.5% in the placebo + ASA group), mainly in the gastrointestinal tract (3.5% vs. 1.8%). There was an excess of intracranial bleeding in the clopidogrel + ASA treatment group compared to the placebo + ASA group (1.4% versus 0.8%. respectively). There was no statistically significant difference in the rates of fatal bleeding (see Table 3) and haemorrhagic stroke (0.8% and 0.6%, respectively) between groups. (See Table 3.)
Click on icon to see table/diagram/image
Haematological disorders: In CAPRIE, severe neutropaenia (<0.450G/L) was observed in 4 patients (0.04%) on clopidogrel and 2 patients (0.02%) on ASA.
Two of the 9599 patients who received clopidogrel and none of the 9586 patients who received ASA had neutrophils counts of zero. Although the risk of myelotoxicity with clopidogrel appears to be quite low, this possibility should be considered when a patient receiving clopidogrel demonstrates fever or other sign of infection.
One case of aplastic anaemia occurred on clopidogrel treatment. The incidence of severe thrombocytopaenia (<80 g/L.) was 0.2% on clopidogrel and 0.1% on ASA; very rare cases of platelet count ≤30 g/L have been reported. In CURE and CLARITY, the number of patients with thrombocytopenia or neutropenia was similar in both groups. Other clinically relevant adverse drug reactions pooled from CAPRIE and CURE, CLARITY, COMMIT and ACTIVE-A198 studies with an incidence <0.1% as well as all serious and relevant ADR with an incidence <0.1% are presented as follows.
The following CIOMS frequency rating is used, when applicable.
Very common ≥10%; Common ≥1 and <10%; Uncommon ≥0.1 and <1%; Rare ≥0.01 and <0.1%; Very rare <0.01%; Unknown (cannot be estimated from available data).
Central and peripheral nervous system disorders: Uncommon: headache, dizziness, paraesthesia. Rare: vertigo.
Gastrointestinal system disorders: Common: dyspepsia, abdominal pain, diarrhoea. Uncommon: nausea, gastritis, flatulence, constipation, vomiting, gastric ulcer, duodenal ulcer.
Platelet, bleeding and clotting disorders: Uncommon: bleeding time increased, platelets decreased.
Skin and appendages disorders: Uncommon: rash, pruritus.
White cell and RES disorders: Uncommon: leucopenia, neutrophils decreased, eosinophilia.
Post-marketing experience: Adverse reactions have been ranked under heading of system-organ class. Frequencies for the following adverse reactions are not known (cannot be estimated from available data).
Blood and the lymphatic system disorders: Serious cases of bleeding, mainly skin, musculoskeletal, eye (conjunctival, ocular, retinal) and respiratory tract bleeding, epistaxis, haematuria and haemorrhage of operative wound; cases of bleeding with fatal outcome (especially intracranial, gastrointestinal and retroperitoneal haemorrhage), agranulocytosis, aplastic anaemia/pancytopenia, thrombotic thrombocytopenic purpura (TTP), acquired haemophilia A.
Immune system disorders: Anaphylactoid reactions, serum sickness; Cross-reactive drug hypersensitivity among thienopyridines (such as ticlopicline, prasugrel) (see Precautions).
Psychiatric disorders: Confusion, hallucinations.
Nervous system disorders: Taste disturbances.
Vascular disorders: Vasculitis, hypotension.
Respiratory, thoracic and mediastinal disorders: Bronchospasm, interstitial pneumonitis, eosinophilic pneumonia.
Gastrointestinal disorders: Colitis (including ulcerative or lymphocytic colitis), pancreatitis, stomatitis.
Hepato-biliary disorders: Hepatitis (non-infectious), acute liver failure.
Skin and subcutaneous tissue disorders: Maculopapular, erythematous or exfoliatiye rash, urticaria, pruritus, angioederna, bultous dermatitis (erythema multitorme, Stevens Johnson syndrome, toxic epidermal necrolysis), drug-induced hypersensitivity syndrome, drug rash with eosinophilia and systemic symptoms (DRESS), eczema, lichen planus.
Musculoskeletal, connective tissue and bone disorders: Arthralgia, arthritis, myalgia.
Renal and urinary disorders: Glomerulopathy.
General disorders and administration site conditions: Fever.
Investigations: Abnormal liver function test, blood creatinine increase.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image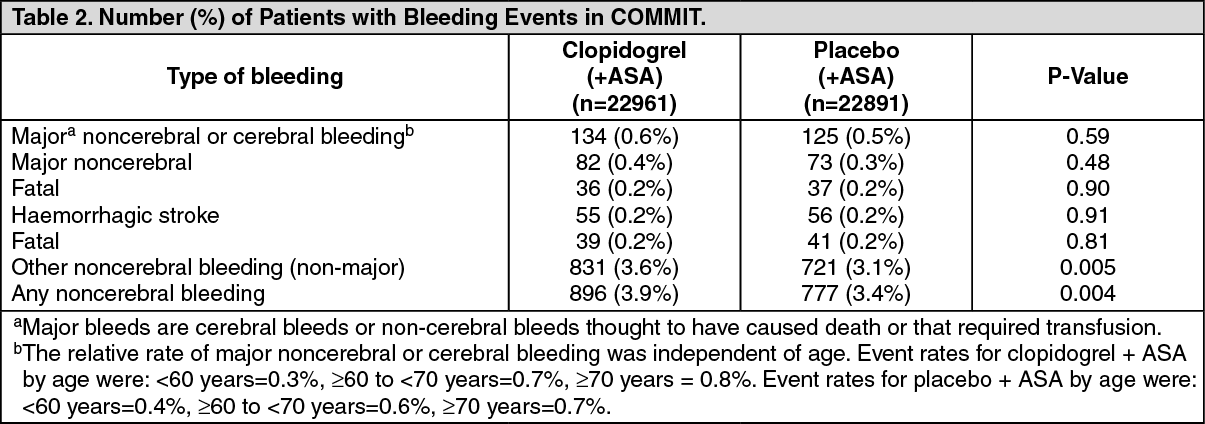 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image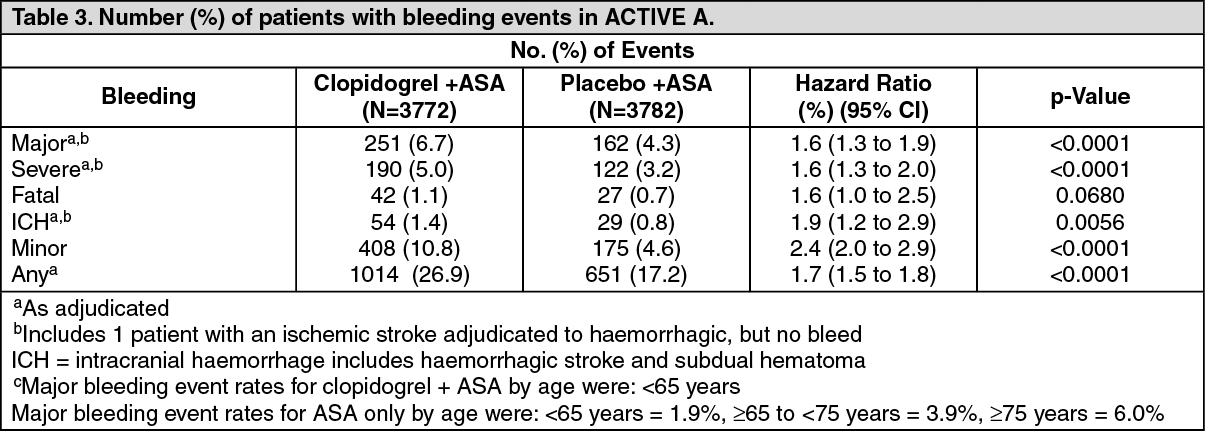 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out